
Dr Victor Chang – The Australian Magazine
A wonderful article from The Australia Magazine on Dr Victor Chang. This was at a time when Dr Chang was leading an international team towards a development of an artificial heart. The aim was that patients could survive on the artificial heart (or ‘Artheart’) until a heart transplant was available.
View the full article here, or read the text below:

THE PATIENT IS LYING ON his back, eyes closed, the life-giving machines blinking and humming in the bright light. Wires taped to his chest pick up a racing heartbeat, yet the heart is no longer sustaining life. Its job is being done by a small, cone-shaped device strapped to his stomach.
It is an artificial heart, pumping life at 80 beats a minute.
Within days, the man will sit up, eat, talk — and watch his own blood flow from the plastic heart, through the tubing and into his body, bypassing his own useless heart, still beating in its place but redundant.
This is not fantasy. Before long, it will become a typical hospital scene, following the successful construction of an artificial heart by Dr Victor Chang and his team of researchers at St Vincent's Hospital in Sydney. Dr Chang, the pioneer of Australia’s successful heart transplant program, sees the heart becoming a standard piece of equipment in cardiac surgical units.
After three years’ research and five prototypes, Dr Chang believes his heart is the most economical (he dislikes the word “cheap”) and the best in the world.
Working with a small Australian engineering company, and one of the best medical brains in China — the surgeon who designed and built China’s heart-lung machine — Dr Chang's team solved problems insurmountable to others, and has successfully completed a series of animal experiments with their heart.
The Australian heart differs from its predecessors, the best-known being the US-built Jarvik-7, which sits inside the chest and replaces the natural heart. The Australian heart sits outside the body and does part or all of the work of the natural heart, but does not physically replace it.
The Australian heart will enable patients to survive for a limited period, possibly for months, while they await a heart transplant (almost 20 per cent of people on the waiting list die before their turn comes). Or it can be used to allow the natural heart to recover after being “stunned” by severe injury to the heart muscle due to inflammation or heart attack, and following cardiac surgery when the patient’s heart muscle temporarily fails to work even though the operation was successful.
Dr Chang's ambitious project has its roots in one of his frequent visits to China. There, in 1977, he saw many people with rheumatic valvular heart disease who would die because they could not afford a heart valve made in America or in Europe. “There are many poor countries and poor people who cannot afford to have the operation,” he says. “I decided then that I would one day create a valve that was affordable.”
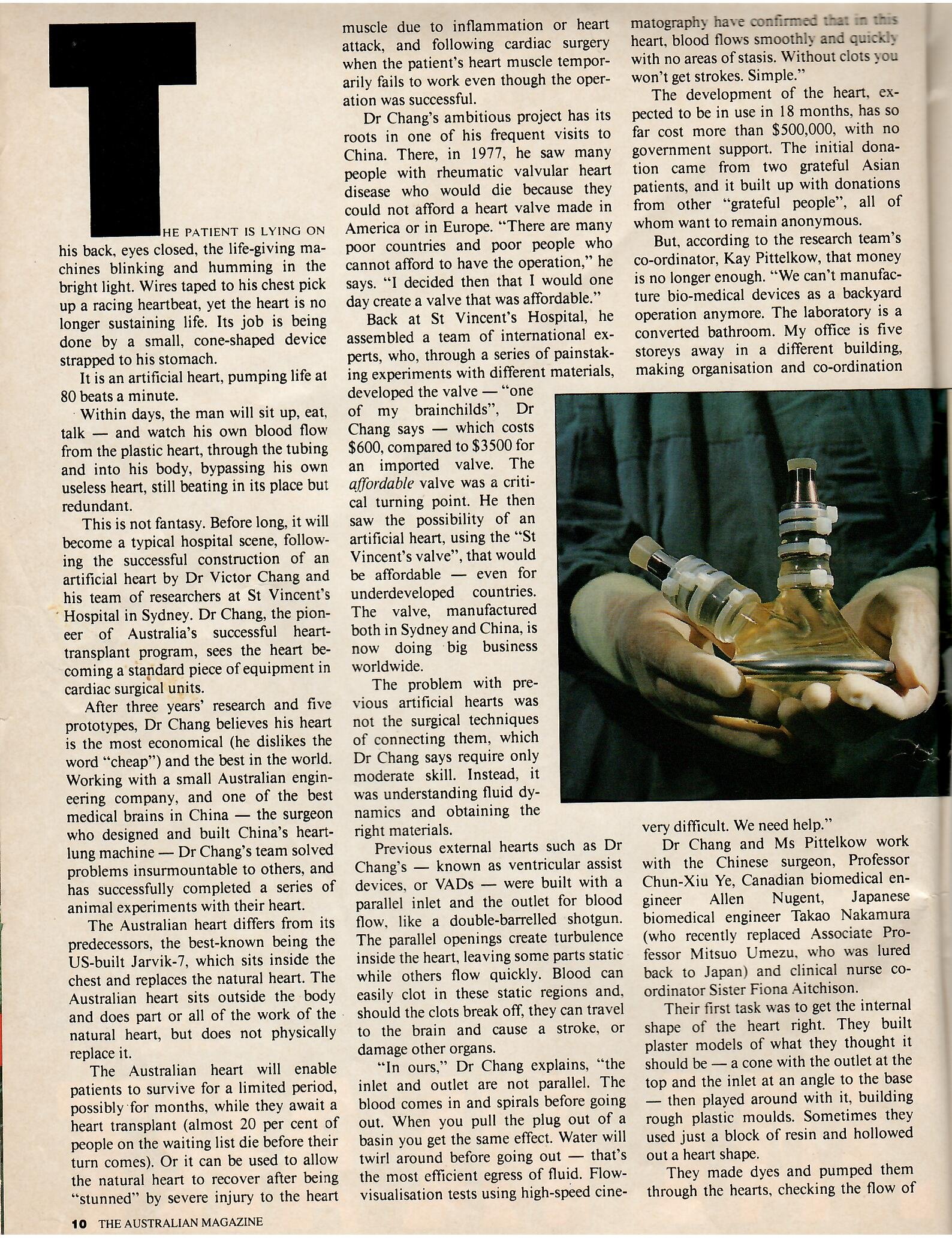
Back at St Vincent's Hospital, he assembled a team of international experts, who, through a series of painstaking experiments with different materials, developed the valve….. — “one of my brainchilds”, Dr Chang says — which costs $600, compared to $3500 for an imported valve. The affordable valve was a critical turning point. He then saw the possibility of an artificial heart, using the “St Vincent's valve”, that would be affordable — even for underdeveloped countries.
The valve, manufactured both in Sydney and China, is now doing big business worldwide.
The problem with previous artificial hearts was not the surgical techniques of connecting them, which Dr Chang says require only moderate skill. Instead, it was understanding fluid dynamics and obtaining the right materials.
Previous external hearts such as Dr Chang's — known as ventricular assist devices, or VADs — were built with a parallel inlet and the outlet for blood flow, like a double-barrelled shotgun.
The parallel openings create turbulence inside the heart, leaving some parts static while others flow quickly. Blood can easily clot in these static regions and should the clots break off, they can travel to the brain and cause a stroke, or damage other organs.
“In ours,” Dr Chang explains, “the inlet and outlet are not parallel. The blood comes in and spirals before going out. When you pull the plug out of a basin you get the same effect. Water will twirl around before going out — that’s the most efficient egress of fluid. Flow-visualisation tests using high-speed cinematography have confirmed that in this heart, blood flows smoothly and quickly with no areas of stasis. Without clots you won't get strokes. Simple.”
The development of the heart, expected to be in use in 18 months, has so far cost more than $500,000, with no government support. The initial donation came from two grateful Asian patients, and it built up with donations from other “grateful people”, all of whom want to remain anonymous.
But, according to the research team’s co-ordinator, Kay Pittelkow, that money is no longer enough. “We can’t manufacture bio-medical devices as a backyard operation anymore. The laboratory is a converted bathroom. My office is five storeys away in a different building, making organisation and co-ordination very difficult. We need help.”
Dr Chang and Ms Pittelkow work with the Chinese surgeon, Professor Chun-Xiu Ye, Canadian biomedical engineer Allen Nugent, Japanese biomedical engineer Takao Nakamura (who recently replaced Associate Professor Mitsuo Umezu, who was lured back to Japan) and clinical nurse co-ordinator Sister Fiona Aitchison.
Their first task was to get the internal shape of the heart right. They built plaster models of what they thought it should be — a cone with the outlet at the top and the inlet at an angle to the base — then played around with it, building rough plastic moulds. Sometimes they used just a block of resin and hollowed out a heart shape.
They made dyes and pumped them through the hearts, checking the flow of fluid and remodelling the hearts until they got it right. All the information was then fed into a computer, which fine-tuned their model.
A further step was to coat the inner surface of the working model with a graphite/silicon mixture, then pump fluid through. Watching the graphite wash off the surface allowed them to see if there would be any areas of stasis near the walls of the heart, which would allow clots to form.
The third main step was to test this device with blood. The team found that their heart damaged the blood only half as much as existing hearts.
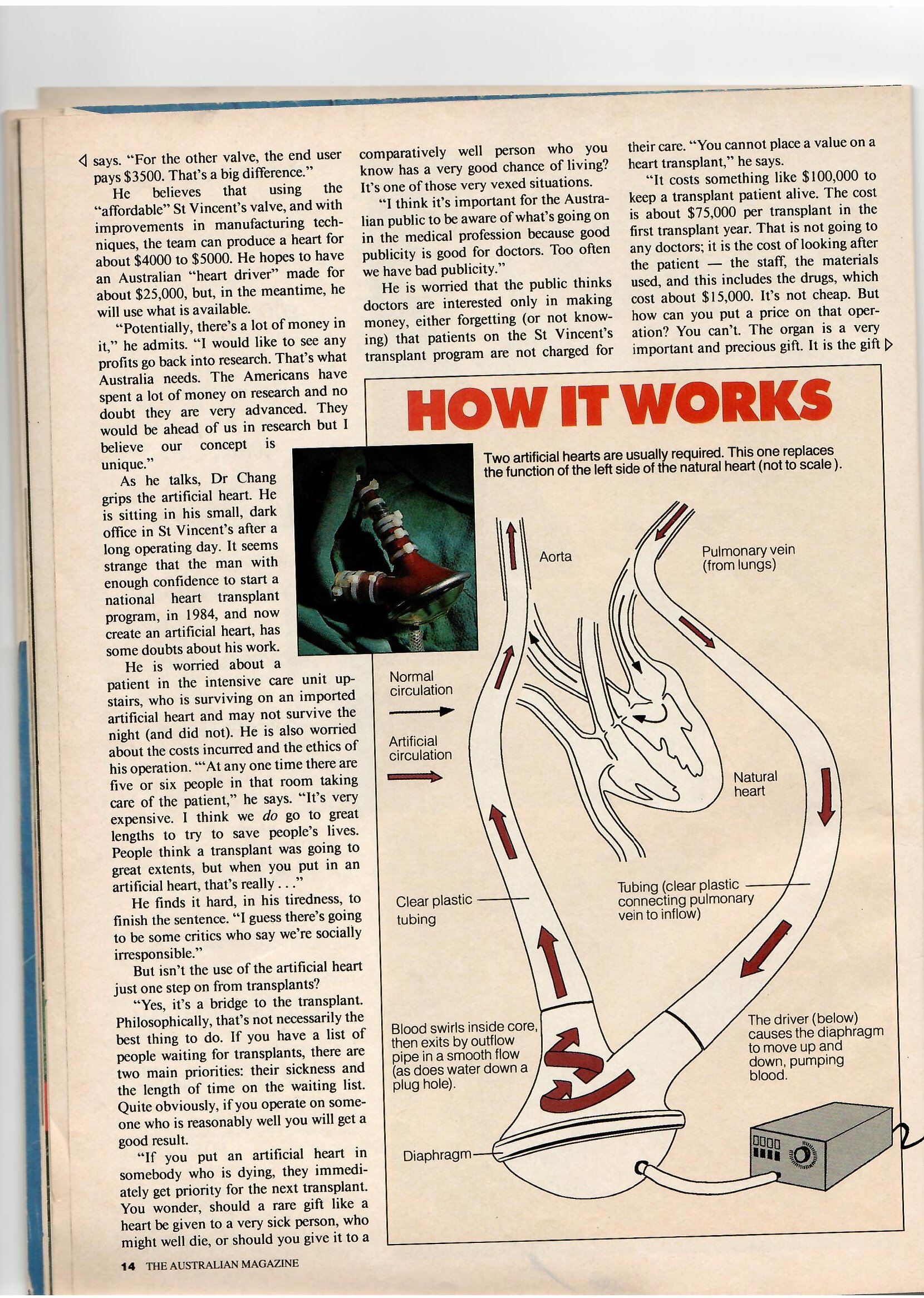
In most cases, each patient will require two artificial hearts. The natural heart is really two separate systems: the right side pushes blood through the lungs to pick up oxygen and the left side pumps it through the body, delivering that dissolved gas to the tissues.
With the St Vincent's artificial heart, two plastic tubes attached to it are grafted to the arteries and veins near the natural, but failing heart. Blood returning along the major veins from the limbs is diverted into a tube which carries it outside the body to the artificial heart. The heart pumps it back up another tube into the lungs. where it picks up oxygen. On its way from the lungs to the left side of the natural heart. it is diverted down a tube to the second artificial heart where it is again pumped. this time at a greater pressure, back into the aorta for its trip through the body tissues.
The driving force for the artificial hearts comes from two large metal boxes beside the bed. Each is attached to the base of the artificial heart by a tube through which the compressor forces air into the heart and then sucks it out, creating a vacuum.
A flexible diaphragm, made of segmented polyurethane, separates the air and blood compartments. Because the casing of the heart is rigid, when air is forced in, the diaphragm moves up, pumping blood out. When a vacuum is created the diaphragm moves down, drawing blood in. One-way valves on the inlet and outlet prevent blood going the wrong way.
The heart and tubing are made of a special plastic which has been used before and is known to be safe.
A material was needed to coat the inside of the heart which would prevent blood clotting. They found the answer in Japan — new chemicals called TM3 and TMS5 were made available to Chang only because of the Japanese researchers in the team.
Dr Chang's team worked with designers, manufacturers and suppliers from the start, with the cost of materials and production paramount. Talon Technology, a small design and engineer business in Sydney, has been moulding the heart. One difficulty faced in other hearts was to get a strong, smooth material that was clear so it could be seen if blood clots were forming or the diaphragm had a tear. Talon did what nobody else in the world had done. It incorporated carbon fibre inserts into the areas of stress, giving the team an unbreakable but transparent heart.
An example of the way the team kept the costs down was in making the dies for the manufacturing diaphragms. “Instead of designing custom and expensive dies, we’ve used ashtray technology” Pittelkow says. “Talon made five quality dies very cheaply using the technologies they use in making ashtrays.”
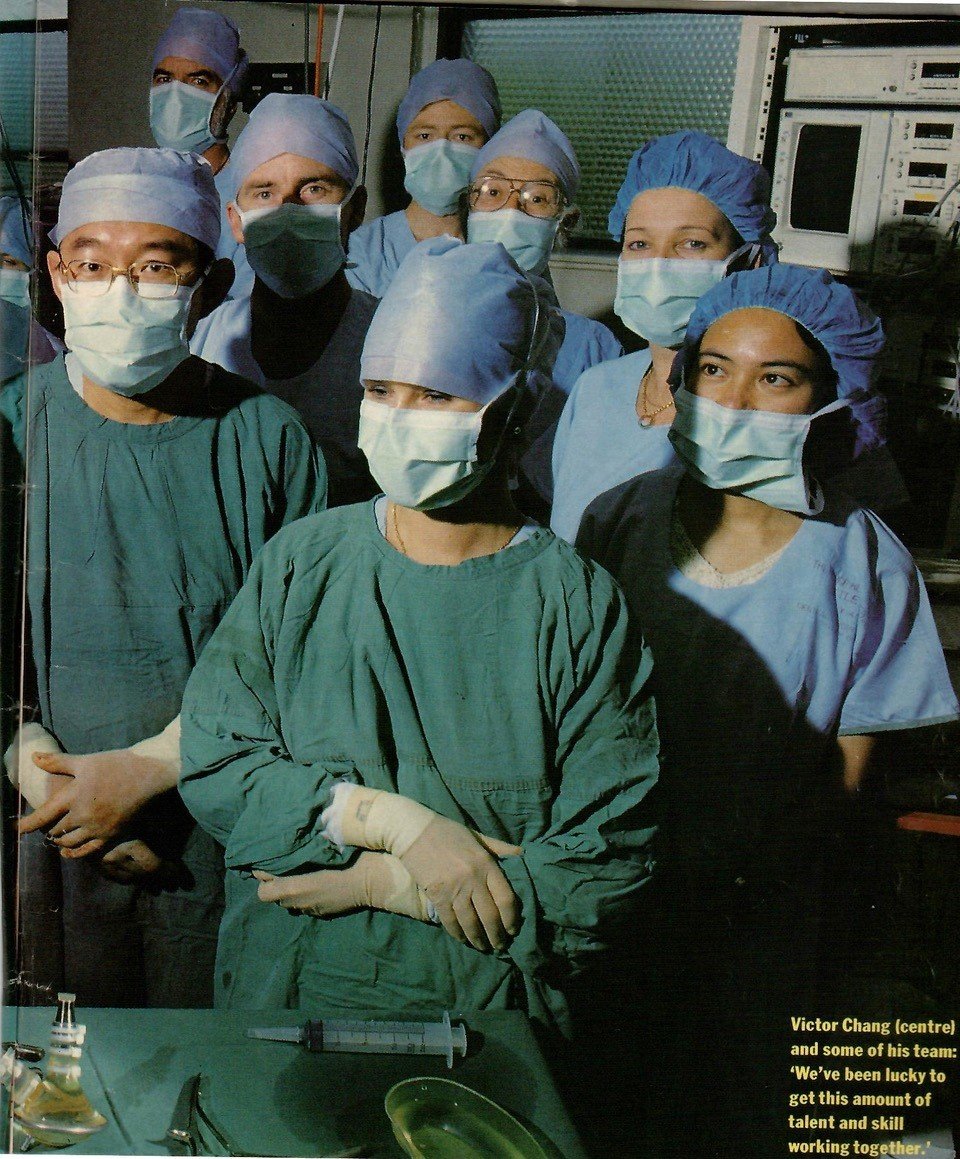
She says the project has quickly compared to other research projects. “We've been lucky amount of talent and skill working together. For example Professor Ye, who actually developed a heart-lung machine in China, could still be working as a brilliant surgeon and saving lots of lives with his hands, but he says that if this heart succeeded, then he would save far more lives with his head.
“The main thing to think of is that with this, people can walk away healthy. People think that high technology medicine is only about delaying death, but with this heart we're talking about getting people back to full health.”
Artificial hearts have a long history, even longer than heart transplants.
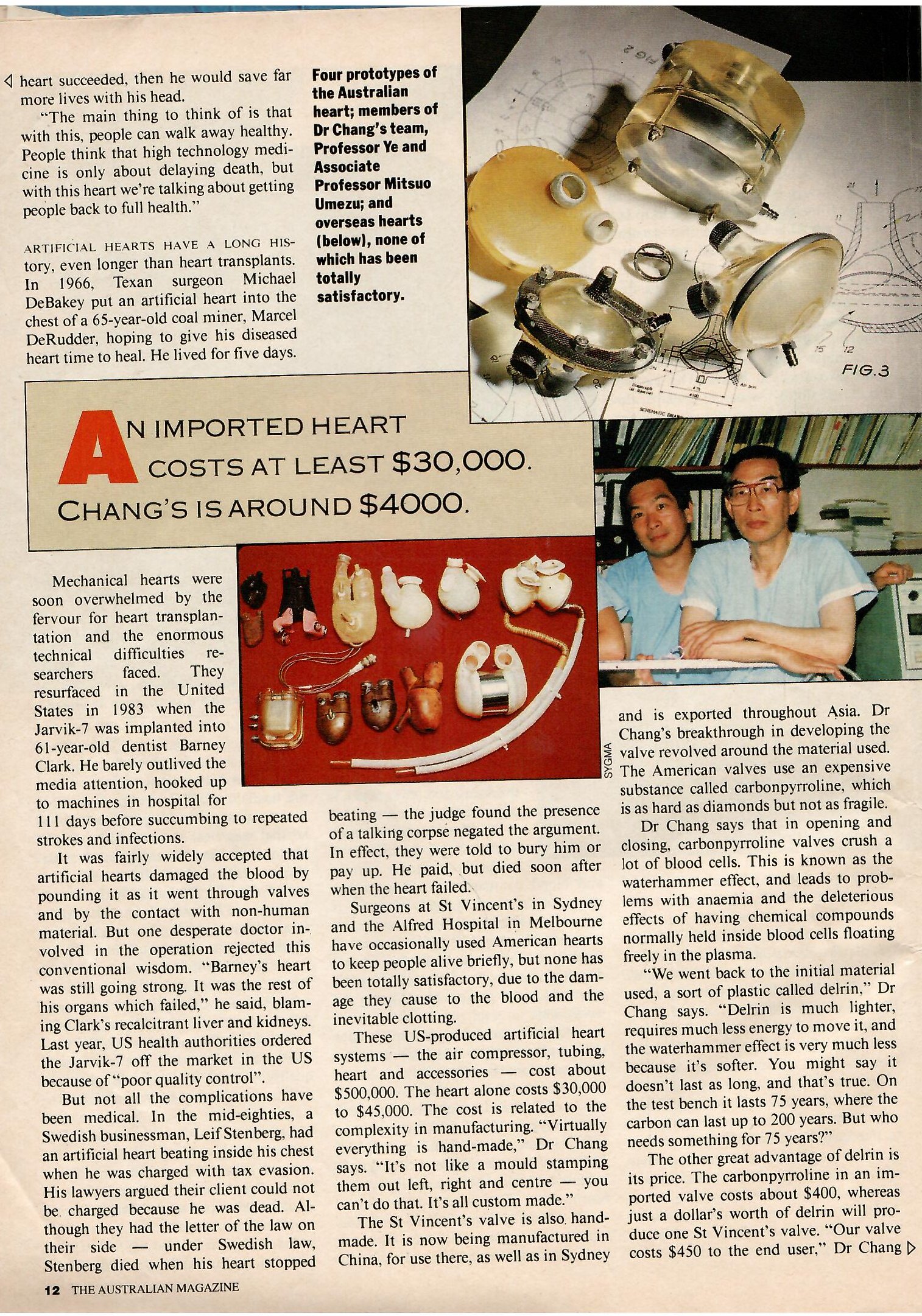
In 1966, Texan surgeon Michael DeBakey put an artificial heart into the chest of a 65-year-old coal miner, Marcel DeRudder, hoping to give his diseased heart time to heal. He lived for five days.
Mechanical hearts were soon overwhelmed by the fervour for heart transplantation and the enormous technical difficulties researchers faced. They resurfaced in the United States in 1983 when the Jarvik-7 was implanted into 61-year-old dentist Barney Clark. He barely outlived the media attention, hooked up to machines in hospital for 111 days before succumbing to repeated strokes and infections.
It was fairly widely accepted that artificial hearts damaged the blood by pounding it as it went through valves and by the contact with non-human material. But one desperate doctor involved in the operation rejected this conventional wisdom. “Barney’s heart was still going strong. It was the rest of his organs which failed,” he said, blaming Clark’s recalcitrant liver and kidneys. Last year, US health authorities ordered the Jarvik-7 off the market in the US because of “poor quality control”.
But not all the complications have been medical. In the mid-eighties, a Swedish businessman, Leif Stenberg, had an artificial heart beating inside his chest when he was charged with tax evasion. His lawyers argued their client could not be. charged because he was dead. Although they had the letter of the law on their side — under Swedish law, Stenberg died when his heart stopped beating — the judge found the presence of a talking corpse negated the argument. In effect, they were told to bury him or pay up. He paid, but died soon after when the heart failed.
Surgeons at St Vincent's in Sydney and the Alfred Hospital in Melbourne have occasionally used American hearts to keep people alive briefly, but none has been totally satisfactory, due to the damage they cause to the blood and the inevitable clotting.
These US-produced artificial heart systems — the air compressor, tubing, heart and accessories — cost about $500,000. The heart alone costs $30,000 to $45,000. The cost is related to the complexity in manufacturing. “Virtually everything is hand-made,” Dr Chang says. “It’s not like a mould stamping them out left, right and centre — you can’t do that. It’s all custom made.”
The St Vincent's valve is also handmade. It is now being manufactured in China, for use there, as well as in Sydney and is exported throughout Asia. Dr Chang's breakthrough in developing the valve revolved around the material used. The American valves use an expensive substance called carbonpyrroline, which is as hard as diamonds but not as fragile.
Dr Chang says that in opening and closing, carbonpyrroline valves crush a Jot of blood cells. This is known as the waterhammer effect, and leads to problems with anaemia and the deleterious effects of having chemical compounds normally held inside blood cells floating freely in the plasma.
“We went back to the initial material used, a sort of plastic called delrin,” Dr Chang says. “Delrin is much lighter, requires much less energy to move it, and the waterhammer effect is very much less because it's softer. You might say it doesn’t last as long, and that’s true. On the test bench it lasts 75 years, where the carbon can last up to 200 years. But who needs something for 75 years?”
The other great advantage of delrin is its price. The carbonpyrroline in an imported valve costs about $400, whereas just a dollar's worth of delrin will produce one St Vincent's valve. “Our valve costs $450 to the end user,” Dr Chang says. “For the other valve, the end user pays $3500. That's a big difference.”
He believes that using the “affordable” St Vincent's valve, and with improvements in manufacturing techniques, the team can produce a heart for about $4000 to $5000. He hopes to have an Australian “heart driver” made for about $25,000, but, in the meantime, he will use what is available.
“Potentially, there’s a lot of money in it,” he admits. “1 would like to see any profits go back into research. That's what Australia needs. The Americans have spent a lot of money on research and no doubt they are very advanced. They would be ahead of us in research but I believe our concept is unique.”
As he talks, Dr Chang grips the artificial heart. He is sitting in his small, dark office in St Vincent's after a long operating day. It seems strange that the man with enough confidence to start a national heart transplant program, in 1984, and now create an artificial heart, has some doubts about his work.
He is worried about a patient in the intensive care unit upstairs, who is surviving on an imported artificial heart and may not survive the night (and did not). He is also worried about the costs incurred and the ethics of his operation. ““At any one time there are five or six people in that room taking care of the patient,” he says. “It’s very expensive. I think we do go to great lengths to try to save people’s lives. People think a transplant was going to great extents, but when you put in an artificial heart, that’s really...”
He finds it hard, in his tiredness, to finish the sentence. “I guess there’s going to be some critics who say we're socially irresponsible.”
But isn’t the use of the artificial heart just one step on from transplants?
“Yes, it’s a bridge to the transplant. Philosophically, that’s not necessarily the best thing to do. If you have a list of people waiting for transplants, there are two main priorities: their sickness and the length of time on the waiting list. Quite obviously, if you operate on someone who is reasonably well you will get a good result.
“If you put an artificial heart in somebody who is dying, they immediately get priority for the next transplant. You wonder, should a rare gift like a heart be given to a very sick person, who might well die, or should you give it to a comparatively well person who you know has a very good chance of living? It’s one of those very vexed situations.
“I think it’s important for the Australian public to be aware of what’s going on in the medical profession because good publicity is good for doctors. Too often we have bad publicity.”
He is worried that the public thinks doctors are interested only in making money, either forgetting (or not knowing) that patients on the St Vincent's transplant program are not charged for their care. “You cannot place a value on a heart transplant,” he says.
“It costs something like $100,000 to keep a transplant patient alive. The cost is about $75,000 per transplant in the first transplant year. That is not going to any doctors; it is the cost of looking after the patient — the staff, the materials used, and this includes the drugs, which cost about $15,000. It’s not cheap. But how can you put a price on that operation? You can’t. The organ is a very important and precious gift. It is the gift of life. It benefits not only the recipient; it also benefits the community generally as that feeling of goodwill from such generosity is generated to all who come in contact with the transplant procedure.”
In other interviews Dr Chang has given, and there are not many, he has played down his achievements. On lung transplants, in 1988, he said: “It’s nothing spectacular. It’s just taking a lung out and putting a new one in.”
Last year, he said: “Heart transplantation in Australia has become just another treatment. There is nothing glamorous or special about heart transplants anymore.”
Of his latest brainchild, Dr Chang says: “I’ve always been very mechanically minded. I enjoy tinkering with things. Mind you, this is not entirely my idea. I’ve got good people working with me. We toss ideas around and then we come up with something.”
He decided from the outset to involve only Australian companies in the heart’s production. “Ultimately it will be an all-Australian product,” he says. “That’s what I want. We should be able to stand up and say, ‘We can do all those things in Australia’.”
THE BEAT GOES ON
May 1953: First successful open-heart surgery, to correct a hole in the heart, performed by John Gibbon at America’s Mayo Clinic. In March 1953, Clarence Denis in New York did a similar operation, but the patient subsequently died of other causes and the surgeon never received the credit he deserved.
March 1957: Australia’s first open-heart surgery using cardiopulmonary bypass to repair a hole in the heart, performed by Ken Morris at The Alfred Hospital, Melbourne.
November 1957: Two great US surgeons, Henry Bahnson and Frank Spencer, from Johns Hopkins Hospital in Baltimore, visit Royal Prince Alfred Hospital, Sydney, and perform 10 open-heart operations, all of which are successful.
1966, Texas: Marcel DeRudder, 65, has an artificial heart implanted inside his body. He lives for five days.
December 3, 1967: In Cape Town, Dr Christiaan Barnard transplants the heart of a young woman killed in a car accident into 55-year-old Louis Washkansky, who dies after 18 days.
October, 1968: Dr Harry Windsor performs Australia’s first heart transplant. The middle-aged man died from infection after six weeks.
1980: The anti-rejection drug cyclosporin becomes available, making transplants infinitely more feasible.
February 1982: In the US, 61-year-old dentist Dr Barney Clark becomes the first man to survive the immediate post-operative period with an artificial heart, living for 111 days in hospital.
February 1984: Dr Victor Chang performs Australia’s first heart transplant of the modern era by giving new life to a 39-year-old South Australian shearer, Peter Apthorpe.
August 1986: Aged 54, William Schroeder dies in the US after 20 months on the Jarvik-7, making him the longest survivor in the history of artificial hearts.
December 1989: One-year-old Heidi Gellert becomes Australia’s youngest heart-transplant recipient.